Is it the dull, nagging ache that makes sitting at your desk a misery? Or the sharp, electric jolt that shoots down your leg without warning?
Back pain isn’t just one thing. It speaks in different languages—a dull throb, a sharp stab, a burning line. And that language holds the clue to its source.
As a pain specialist, I’ve learned that the most empowering first step for any patient is putting a name to their pain. It’s the moment you stop being a victim of a mysterious ache and start becoming an active detective in your own relief. Understanding the different types of back pain is the key that unlocks a more intelligent conversation with your doctor and a more effective path forward.
This guide will help you decode the signals your body is sending.
Key Takeaways: How to Know Your Type of Back Pain
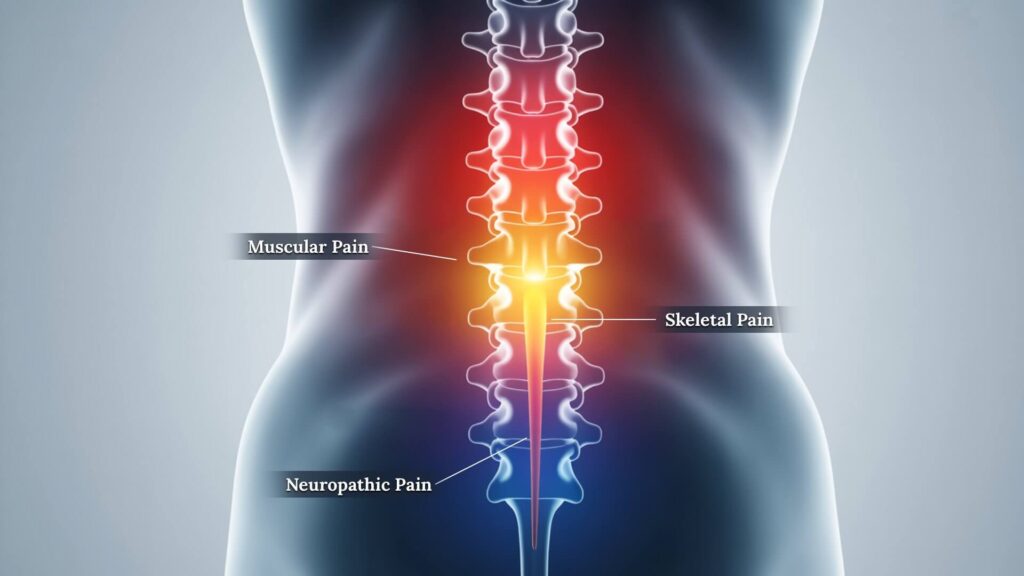
- Muscular Pain: Feels like a dull, aching soreness, often with muscle spasms. It’s usually caused by overuse or poor posture and feels better with rest. The pain stays in the back.
- Skeletal / Structural Pain: A deeper, sharper pain linked to specific movements (like bending forward). It suggests an issue with the discs or bones of the spine.
- Neuropathic Pain: Has a distinct burning, tingling, or “electric shock” quality. The key clue is that the pain radiates or shoots down your leg (like sciatica).
- When to See a Doctor: While this guide helps you understand your symptoms, it’s not a diagnosis. If your pain is severe, persistent, or accompanied by “red flag” symptoms (like weakness or loss of bladder control), a professional evaluation is essential.
Table of Contents
Prefer to Listen? An Audio Overview
For a conversational deep dive into this topic, press play below for the complete audio discussion with our hosts.
Runtime: 3 minutes
View Full Audio Transcript
Narrator: Welcome. Today we’re decoding back pain. Dr. Emily, the number one question our listeners have is, “How do I know what type of back pain I have?” Why is that distinction so important?
Dr. Emily Richards: It’s the most critical first step. “Back pain” isn’t one thing. Understanding if the signal is coming from your muscles, your bones, or your nerves is the key that unlocks a more effective treatment plan and a better conversation with your doctor.
Narrator: Let’s start with the most common type. How can someone know if their pain is muscular?
Dr. Emily Richards: Muscular pain is typically a dull, aching soreness. You might get sharp spasms, but the core feeling is an ache. The key clue is that it’s often linked to an activity—like overdoing it in the garden—and it usually feels better with rest or gentle stretching. Crucially, the pain tends to stay localized in the back muscles.
Narrator: Okay, but what if it’s not a dull ache? How can someone tell if their back pain is a more serious muscle or disc issue?
Dr. Emily Richards: That’s the next level of detection. When the pain is skeletal or structural, coming from the discs and bones, it feels deeper and sharper. The pain is often directly tied to a specific position. For example, pain that gets much worse when you bend forward can point to a disc issue. Pain that feels better when you lean forward, like over a grocery cart, is a classic clue for spinal stenosis.
Narrator: That’s a very clear distinction. Now for the third type, neuropathic pain. What does neuropathic back pain feel like?
Dr. Emily Richards: Neuropathic pain speaks a completely different language. Patients use words like burning, tingling, shooting, stabbing, or an electric shock. The absolute defining characteristic is that the pain radiates. It doesn’t stay put. It travels from the lower back, down the buttock, and into the leg. Sciatica is the most famous example of neuropathic pain.
Narrator: And is it common for these types to overlap?
Dr. Emily Richards: Extremely common—in fact, it’s the norm. A herniated disc is a perfect example. The disc itself causes deep, skeletal pain. This can trigger the surrounding muscles to spasm in protection, causing muscular pain. And if that disc presses on a nerve root, it will cause radiating neuropathic pain. All three types from one single problem.
Narrator: So, what’s the main takeaway for someone trying to figure this out?
Dr. Emily Richards: Become a detective of your own pain. Your job isn’t to self-diagnose, but to gather clues. Pay attention to the language of your pain—is it aching, sharp, or burning? What makes it better or worse? Bring this information to your doctor. It will transform the quality of your care and set you on the right path to relief.
1. Muscular Pain (The Most Common Culprit)
This is the type of back pain most people are familiar with. It involves the muscles, ligaments, and tendons that support your spine.
- What It Feels Like: Typically described as a dull, aching, or sore feeling. It can be localized to one area or feel like a general stiffness across the lower or upper back. You might also experience sharp muscle spasms.
- Common Causes: Overuse (like a long day of yard work), lifting a heavy object improperly, poor posture (especially sitting at a desk), or a sudden awkward movement.
- The Key Clue: Muscular pain often feels better with rest and gentle stretching. It may feel worse with specific movements but doesn’t usually cause pain to radiate far down your leg.
2. Skeletal / Structural Pain (Bone & Joint Issues)
This type of pain originates from the bones of the spine (vertebrae) and the discs that cushion them.
- What It Feels Like: Often a deeper, sharper, and more localized pain than muscular aches. It can be a constant, nagging pain that worsens significantly with specific movements like bending forward, twisting, or standing for long periods.
- Common Causes: Herniated discs, spinal stenosis (a narrowing of the spinal canal), or arthritis of the spine (spondylosis).
- The Key Clue: The pain is strongly linked to specific positions. Pain that is worse when you bend forward might suggest a disc issue, while pain that feels better when you lean forward (like over a shopping cart) can be a clue for spinal stenosis.
3. Neuropathic Pain (Nerve-Related Pain)
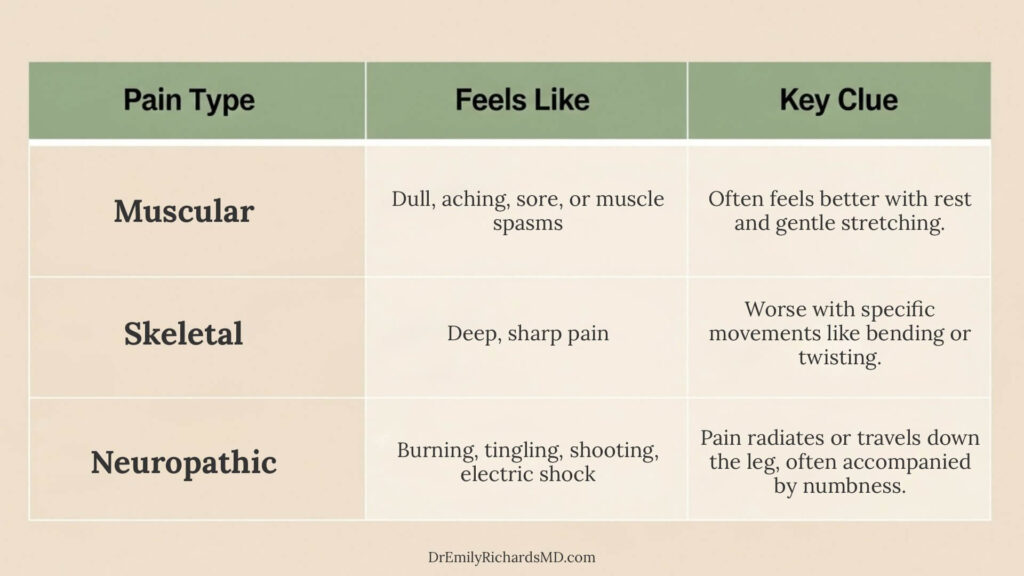
| Characteristic | 1. Muscular Pain | 2. Skeletal / Structural Pain | 3. Neuropathic Pain |
|---|---|---|---|
| What It Feels Like | Dull, aching, sore, stiff, muscle spasms. | Deep, sharp, nagging, localized. | Burning, tingling, shooting, electric shock. |
| Key Clue / Location | Stays in the back muscles; feels better with rest. | Linked to specific positions (e.g., bending forward). | Radiates from the back down the leg (sciatica). |
| Common Causes | Overuse, poor posture, muscle strain. | Herniated disc, arthritis, spinal stenosis. | Pinched or irritated nerve, often from a skeletal issue. |
Neuropathic pain is caused by irritation, compression, or damage to the nerves themselves as they exit the spinal column.
- What It Feels Like: This is the most distinct type of pain. Patients often use very specific words to describe it: burning, tingling, shooting, stabbing, or like an electric shock. Sciatica is the classic example.
- Common Causes: It is often a result of a skeletal problem. For example, a herniated disc can press directly on a nerve root, causing neuropathic pain. The mind-body connection also plays a crucial role in the experience of neuropathic pain.
- The Key Clue: The pain radiates. It doesn’t stay in one spot. It often travels or “shoots” from the lower back down the buttock and into the leg, sometimes all the way to the foot. Numbness or weakness in the leg can also be present.
The Overlap: It’s Often a Combination
Here’s a truth from 15 years in clinical practice: back pain rarely fits into a neat little box. More often, it’s a messy combination platter. A structural problem, like a herniated disc (skeletal), can trigger a cascade of effects: it causes protective muscle spasms (muscular) and can simultaneously irritate a nearby nerve root (neuropathic). This overlap is precisely why a comprehensive diagnosis is so vital, and why your pain can persist long after the initial event.
What to Do Next: Become a Detective of Your Pain
Your primary goal is to gather information so you can have the most productive conversation possible with your doctor.
- Track Your Symptoms: Note when your pain is better or worse. What time of day? What activities? This helps identify patterns.
- Note the Sensation: Use the descriptive words—aching, burning, sharp, dull—when you talk to your doctor.
- Describe the Function: How does the pain impact your life? Does it stop you from sleeping, walking, or working? This context is crucial.
Understanding the potential source of your pain is not a replacement for a medical diagnosis, but it is the first step toward advocating for yourself and finding the right path to relief, which often includes a variety of proven non-pharmacological strategies.
Frequently Asked Questions
How can I tell if my back pain is muscular or a more serious organ issue, like kidney pain?
This is a critical question. While a doctor’s diagnosis is essential, here’s a key clue: Muscular back pain often changes with movement and position. Kidney pain, however, is typically a deeper, constant ache on one side of the mid-back (flank area) that doesn’t change with your position.
What are “red flag” symptoms for back pain that mean I should see a doctor immediately?
While most back pain is not an emergency, you should seek immediate medical attention if your back pain is accompanied by fever, unexplained weight loss, loss of bladder or bowel control, or progressive weakness or numbness in your legs.
Can I have more than one type of back pain at the same time?
Absolutely. In fact, it’s very common. A structural issue like a herniated disc can cause localized skeletal pain, which then leads to protective muscle spasms (muscular pain) and can also press on a nerve, causing radiating neuropathic pain. This overlap is why a thorough diagnosis is key.
Disclaimer: The content provided by Dr. Emily Richards is for informational and educational purposes only and does not constitute medical advice. Always consult with your healthcare provider for any health concerns or before making any changes to your treatment plan.
References
View Full List of Scientific References
- Dey S, Sanders AE, Martinez S, et al. (2024). Alternatives to Opioids for Managing Pain. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK574543/
- Jensen TS, Finnerup NB. Allodynia and hyperalgesia in neuropathic pain: clinical manifestations and mechanisms. Lancet Neurol. 2014 Sep;13(9):924-35. doi: 10.1016/S1474-4422(14)70102-4. PMID: 25142459. https://pubmed.ncbi.nlm.nih.gov/25142459/
- Mayo Clinic. Back pain – Symptoms and causes. Updated August 29, 2024. Accessed August 29, 2025. https://www.mayoclinic.org/diseases-conditions/back-pain/symptoms-causes/syc-20369906
- Mayo Clinic. Spinal stenosis – Symptoms and causes. Updated August 29, 2024. Accessed August 29, 2025. https://www.mayoclinic.org/diseases-conditions/spinal-stenosis/symptoms-causes/syc-20352961
- Jensen TS, Finnerup NB. Allodynia and hyperalgesia in neuropathic pain: clinical manifestations and mechanisms. Lancet Neurol. 2014 Sep;13(9):924-35. doi: 10.1016/S1474-4422(14)70102-4. PMID: 25142459.
- Mayo Clinic. Sciatica – Symptoms and causes. Updated August 29, 2024. Accessed August 29, 2025. https://www.mayoclinic.org/diseases-conditions/sciatica/symptoms-causes/syc-20377435
- Bratton RL. Assessment and Management of Acute Low Back Pain. Am Fam Physician. 1999;60(8):2299-2306. PMID: 10569602.

Start Healing from the Inside Out
Download my FREE 7-Day Anti-Inflammatory Kickstart Guide. It’s a simple, doctor-designed plan to help you reduce inflammation and soothe pain, one meal at a time.
